


The Role of Lactate
Lactate is an intermediary metabolite of the anaerobic and aerobic biochemical mechanisms responsible for continuous energy supply during exercise. At rest, fats in the form of triglycerides from adipose tissue are the primary fuel when oxygen is freely available from the lungs. At low intensities of exercise, glucose is predominantly metabolised aerobically to meet greater energy needs and enters the Citric acid cycle (also known as Krebs cycle) in the mitochondria of muscles, a process known as oxidative phosphorylation. However, as exercise intensities are increased, the availability of oxygen is insufficient or absent (hypoxia/anoxia) to meet the full energy requirements. At this point, glucose from the blood or glycogen reserves in the muscle and liver are used less efficiently (by Type IIx fast-twitch/glycolytic muscle fibers) to produce energy in the form of ATP. Lactate is produced from the by-product pyruvate, although this is easily re-converted back to glucose in the liver (Cori cycle, shown opposite).

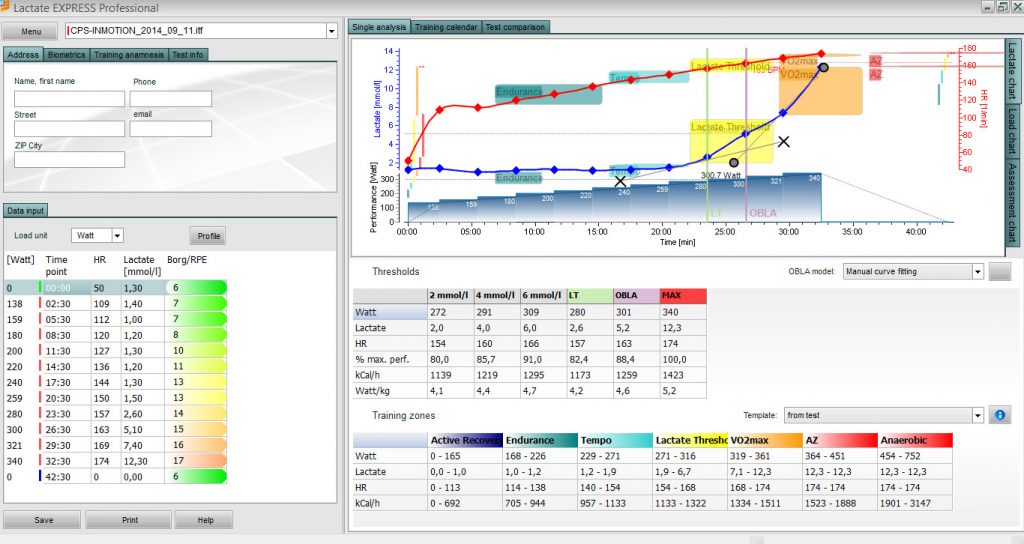
The point at which this lactate recycling is overwhelmed by a further increase in exercise intensity is regarded as the Lactate Threshold or better defined as the lactate turning points. Lactate accumulates along with an associated fall in blood pH (acidity) and results in rapid muscular fatigue and failure. Lactate itself is not considered to be directly responsible for muscle failure and fatigue, and is actually known to be beneficial to energy reserves as a substitute carbohydrate which preserves glucose use, once sufficient oxygen is available for aerobic metabolism (see Excess Post-exercise Oxygen Consumption, EPOC). L.B.Gladden J Physiol 558.1 (2004) 5-30. Read more on the physiology of endurance sport here.
Lactate threshold profiling has fast become the most valuable sports performance assessment, and provides important insight into an athletes ability and unique physiology. More importantly LT profiling allows for critical tracking of fitness during a prescribed block of training, or through the seasons, and serves as an important parameter to many of the Impulse-Response models for performance prediction and is far superior to crude functional estimations of FTP. FTP measurements tend to overestimate the lactate threshold value, due to elevated lactate values throughout, and do not offer the wealth of multple data that a full lactate profile provides.
Lactate therefore considers the inherent mechanical efficiency of a rider (an accurate surrogate for oxygen delivery to, and consumption by the muscles) as the lactate threshold is a function of aerobic metabolic efficiency and expression of key enzymes in the muscle. This highlights the redundancy of erroneous VO2 max testing and indirect methods of determining ventilatory lactate thresholds at inflection points, which only indicates an absolute capacity and is a less sensitive training response marker. The absolute performance value of VO2 max testing is usually only informative when comparing training status with other competitors, something which is fraught with inconsistencies and not appropriate. The proportion of the overall aerobic capacity that a riders lactate threshold is working to (eg 50% for an untrained individual or up to 90% for an elite rider) is informative, but is best understood in absolute terms of a blood lactate profile.

Cyclists from different disciplines will elicit relatively different lactate threshold profiles. Cyclo-cross and criterium racers will produce higher levels of lactate overall, but will not have much higher peak values (above threshold) due to the larger anaerobic capacity and ability to distribute lactate when compared to a time trialist or road racing cyclist, as the aerobic capacity is still conserved. Track cyclists and pure sprinters will demonstrate higher anaerobic capacities and hence higher lactate levels further still. The anaerobic phenotype (inherent expression) of natural sprinters results in greatly elevated levels of lactate which is efficiently metabolised over short durations. The optimal balance of the proportion of anaerobic fibers (Type IIX fast-twitch, glycolytic) to aerobic muscle fibers (Type IA, slow, oxidative) ultimately determines success at the discipline of choice. Therefore, comparison of LTP/LTHR values pre-, mid- and post-training is probably the best method for evaluating an effective training plan.
LT power and average heart-rate at the Maximum Lactate Steady-State (MLSS, see Lactate Profiling) is an accurate measurement of the point at which further anaerobic effort is not sustainable, and is regarded as the approximate ‘1 hour Time Trial effort’. In practice however, the duration of which the sustainable intensity any lactate produced by the muscles is processed by the body without accumulating in the blood, can range between 30-90 minutes between individuals. The Onset of Blood Lactate Accumulation (OBLA), i.e. when lactate uncontrollably accumulates in the blood, usually occurs immediately after MLSS.
Previously, much confusion has existed with the terms used for Lactate Thresholds and turning points cited in much research. The Individual Anaerobic Threshold (IAT) and other definitions of the turning points have made interpretation difficult. Although now it is known that incremental work-rate protocols offer an accurate means to determine MLSS values through objective analysis of the lactate profile, using established methods. Van Schuylenbergh, Int J Sports Med 2004 Aug:25(6):403-8.
A further article originally published by HVMN is available here, which also highlights the benefits of lactate threshold training and role in endurance sport.
The Assessment
An initial consultation and acquires baseline characteristics (demographic variables, age, weight, BMI, sex etc), current and historical training volume and life/work commitments. Resting lactate, blood pressure, weight and body fat analysis are also performed.

The assessment is conducted entirely on your own bike using a laboratory grade static ergometer (CompuTrainer). After an initial warm-up, each athlete initiates the protocol with a tailored starting load e.g. 120 Watts, determined relative to their training status. Blood lactate measurements are easily taken with an accurate portable lactate monitoring device during the last 30 seconds of each three minute power increment (along with relative perceived exertion, heart rate and power data channels). Depending on the riders ability, the power rating is incrementally increased by constant amounts every three minutes, to achieve approximately a full profile of samples before volitional exhaustion is reached by the subject.
The physiological threshold is determined through advanced modelling techniques at which the onset of lactate accumulation, or when lactate clearance is overwhelmed by production, as anaerobic and aerobic metabolisms are no longer in harmony. The average power value or heart rate value (depending on the rider’s use of a power meter or heart rate monitor) can then be converted to the physiologically relevant training zones necessary for following a polarised periodisation programme. The assessment requires informed consent and an initial health screen.
The modelled threshold parameters can then be translated to discrete values for each targeted energy system, well described in current sports science literature for power based intervals of specific durations. These are dynamic power and heart rate ranges and therefore change with training status, which in turn warrants re-assessment usually every 3 – 4 months in full-time working recreational cyclists or runners, as to maintain the progression of sustainable performance improvements, when compliant with a structured training programme.

Blood Lactate Measurements and Analysis during Exercise: A Guide for Clinicians Matthew L. Goodwin, M.A., James E. Harris, M.Ed., Andrés Hernández, M.A., and L. Bruce Gladden, Ph.D. J Diabetes Sci Technol. 2007 Jul; 1(4): 558–569.
Time to move beyond a brainless exercise physiology: the evidence for complex regulation of human exercise performance Timothy David Noakes
Lactate threshold concepts: how valid are they? Faude O, Kindermann W, Meyer T. Sports Med. 2009;39(6):469-90.
How do you compare? – Chris Froome, Physiological report from GSK Human Performance Lab and narrated story here.

